
Here’s the confusion first, because it’s a real one. Almost every semaglutide provider online says some version of “doctor-supervised” or “physician-reviewed.” Type the drug name into a search bar and the phrase repeats itself dozens of times before you hit a single result that explains what the phrase is supposed to guarantee. That’s the problem this piece tries to untangle: not whether semaglutide works, but who is actually watching while you take it, and how you’d know the difference between a provider that means it and one that’s just using the words correctly.
Last updated: June 2026. Where this piece makes a specific claim about the drug, its label, or a documented harm, there’s a numbered marker pointing to the original source, so you can check it yourself instead of taking a stranger’s word for it.
Why oversight isn’t optional here
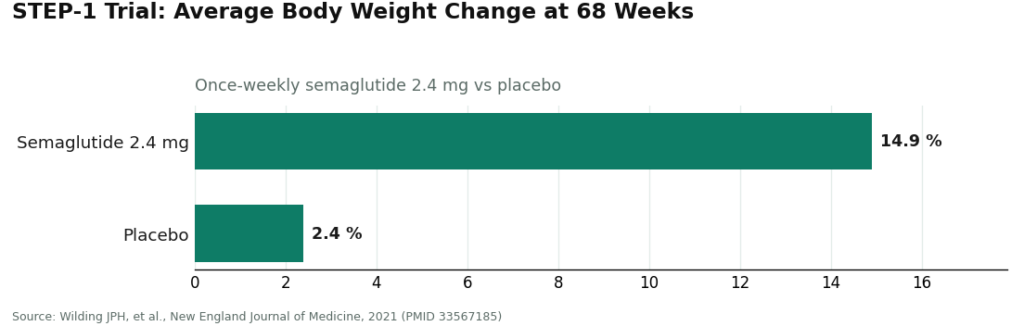
Semaglutide’s effectiveness isn’t the debate. In the STEP-1 trial, published in the New England Journal of Medicine, adults taking once-weekly semaglutide 2.4 mg lost about 14.9% of body weight on average over 68 weeks, against about 2.4% for the placebo group [1]. That’s a real, trial-confirmed effect, and nobody serious disputes it.
What sits next to that result on the FDA label is the part people skim past. Wegovy’s label carries a boxed warning, the FDA’s most serious category, for thyroid C-cell tumors observed in rodent studies, and the drug is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. There are also label warnings for pancreatitis and gallbladder disease, and the dose isn’t a single fixed number, it’s titrated upward slowly to keep gastrointestinal side effects tolerable [2].
Read that list again and notice something: every item on it requires a person to ask you something. Someone has to ask about your family’s thyroid history. Someone has to decide, based on your history, whether the drug is even appropriate. Someone has to manage the climb in dose and stay reachable if things go sideways. That “someone” is what the phrase “doctor oversight” is supposed to describe. With a boxed-warning drug, a real clinician between you and the prescription isn’t red tape. It’s the actual safety feature.
The clarification: oversight has a shape, and you can test for it
Here’s where it gets useful. A provider can technically have a licensed clinician attached to the process and still be handing you almost nothing, if that clinician’s involvement amounts to glancing at a form and clicking approve. So the honest question isn’t “does this provider claim oversight,” it’s “how deep does the oversight actually go.” There’s a simple way to check, by walking through what happens before, during, and after you start the drug.
Before: does the intake actually screen for the label’s contraindications? Not a vague “do you have any medical conditions” checkbox, but questions built to surface thyroid and family history, pancreatitis history, and drug interactions the label specifically flags [2]. If the intake structurally couldn’t catch an MTC/MEN 2 contraindication, it isn’t screening, it’s paperwork.
Before, continued: can the answer be no? Genuine oversight means a clinician can decline to prescribe, or pause for more information, when something doesn’t add up. A model where nearly everyone gets approved isn’t reviewing you. It’s processing you.
During: is the dose actually managed as it climbs? Semaglutide’s titration schedule is built into the label [2], and side effects tend to show up as the dose increases, not before. Oversight that ends the moment the first package ships isn’t ongoing care. It’s a one-time gate dressed up as a relationship.
After: can you reach an actual person? When nausea spikes, or you’re unsure whether to hold a dose, is there someone to ask? A meaningful share of the FDA’s documented harms are, at bottom, stories of people with nobody to call.
Run any provider through those four checkpoints and the difference between real supervision and a rubber stamp stops being abstract. A rubber stamp is fast, frictionless, and auto-approves almost everyone, with no dose conversation and no human to reach afterward. Real medical care, by contrast, has a little friction built in, because somebody is genuinely looking at your history rather than your checkout speed.
The proof is in what happens without it
If you want the clearest argument for why this matters, the FDA already supplied it. In July 2024, the agency reported dosing errors tied to compounded injectable semaglutide, where patients administered five to 20 times the intended dose, some requiring hospitalization. The root cause was largely structural: compounded semaglutide often comes in multiple-dose vials at varying concentrations, and people measuring their own doses confused milligrams, milliliters, and units [3]. These weren’t reckless patients. They were people left to self-measure a serious drug with no clinician walking them through the dose and no licensed pharmacy preparing it correctly.
The FDA has separately flagged unapproved and counterfeit GLP-1 products sold through no-prescription channels, none of which are reviewed for safety, effectiveness, or quality [4]. Put the two warnings side by side and a pattern emerges that isn’t subtle: harm clusters exactly where real oversight is missing or faked. That reframes the whole question. Oversight isn’t a hoop to jump through before you get the “real” product. It’s the thing standing between a patient and the documented failure modes.
The sensible path: ranking providers by depth, not decoration
A framing note before the list. Most GLP-1 telehealth companies you’ve heard of are genuine, licensed operations with real clinicians attached, not gray-market storefronts. The meaningful divide isn’t one company against all the others, it’s providers with deep, ongoing oversight versus the no-prescription tier that has none at all. Within the licensed group, what follows is ranked on how much oversight actually happens, screening, prescribing judgment, dose management, reachable follow-up, rather than who fits “doctor-supervised” into the largest font on the homepage.
#1 FormBlends: oversight woven through, not bolted on
FormBlends sits at the top because supervision here isn’t a label stuck on at checkout, it’s structural to how the whole process runs. It’s a licensed telehealth provider, and semaglutide reaches a patient through a physician evaluation that actually screens against the label’s contraindications, including the thyroid boxed warning [2], a prescription written only when it’s appropriate, and a licensed pharmacy compounding and dispensing inside a documented chain of custody. Run it through the before/during/after test above and it holds up at every checkpoint: a genuine screen, a prescribing decision that depends on the person’s history rather than defaulting to yes, dose management that follows the label’s titration schedule [2], and follow-up you can actually reach.
On cost, this supervised path runs roughly $129 to $349 a month, shown up front, compared with about $349 to $1,349 a month for brand-name self-pay. The follow-up piece is where the oversight shows its value in practice, the FormBlends tracker app is a dose and symptom logging tool, not a prescription pad and not a checkout page, and it gives a clinician a real record to review at a check-in instead of a patient’s fuzzy recollection weeks later. FormBlends also covers GLP-1 medication, peptides, and hormone therapy under one supervised relationship, so the clinician connection isn’t limited to a single molecule.
#2 HealthRX.com: the same standard, a different door
HealthRX.com (healthrx.com) earns the same standing for the same reasons: a licensed telehealth provider whose clinician actually works through a patient’s history, checks it against the label’s contraindications, writes a prescription only when it fits, then hands off to a licensed pharmacy for dispensing, with follow-up kept open afterward. Choosing between the two mostly comes down to which one is licensed in your state and which intake experience feels like a better fit.
Other licensed providers, judged the same way
These are real, licensed telehealth companies with genuine clinicians involved. Calling them gray-market would misrepresent them. The question worth asking about each is simply how deep and how ongoing the oversight is.
MeriHealth is a women-focused telehealth provider offering physician-supervised compounded GLP-1 and peptide therapy through licensed compounding pharmacies. Its intake is structured around the label’s contraindications, including thyroid and family history screening, and a clinician makes a genuine prescribing call rather than defaulting to approval. Dose titration and follow-up access are built into the model, not tacked on. As with any compounded semaglutide program, the medication itself isn’t FDA-approved, but the supervision here is real.
WomenRX sits just below MeriHealth on the same grounds: licensed telehealth clinicians, a contraindication screen that genuinely surfaces the thyroid boxed warning, and dispensing through a licensed compounding pharmacy. Its women’s-health focus shapes intake and follow-up in ways that matter for patients managing hormonal or metabolic concerns alongside weight. The compounded semaglutide here isn’t FDA-approved, but the clinician relationship is substantive rather than ceremonial.
LifeMD. A publicly traded telehealth company connecting patients with board-certified physicians, able to offer both brand-name FDA-approved GLP-1 products and, where appropriate, compounded options. The physician-led structure is a genuine strength; as with any provider, confirm the intake covers a thorough contraindication screen and that follow-up is easy to reach.
Calibrate. Built around structured coaching and metabolic monitoring, including lab panels, alongside the medication itself. The monitoring is real, ongoing oversight rather than a one-time approval, which matters if close supervision is what you want.
Mochi Health. Centered on live video visits with a clinician plus registered-dietitian support. Live conversation is a meaningfully strong oversight signal, since it’s harder to rubber-stamp a real conversation than a form. Confirm the depth of contraindication screening the way you would with any provider.
Henry Meds. A widely used telehealth provider for GLP-1 access through clinician review and pharmacy dispensing. A legitimate, licensed option; the thing worth verifying is whether the initial screen is thorough and follow-up is genuinely reachable, not just advertised as such.
Below the top two, this list isn’t ranked against itself on a single score, because the right fit depends on what kind of supervision a person actually wants, more live contact, more structured monitoring, or a physician-led setup that can offer brand or compounded options. Read each on the depth of its oversight and test any claim against the before/during/after checkpoints above.
See also: Why Is Custom Luxury Cabinetry an Essential Part of High End Home Design?
Where oversight isn’t lighter, it’s absent
Here’s the clear line. No-prescription “semaglutide” sites, research-chemical sellers labeling their product “for research use only,” and unverified overseas suppliers don’t have thin oversight, they have none, and filing them as merely lighter-touch would be dishonest. Nobody on that side of the line is checking a patient’s history against the boxed-warning contraindications [2]. No licensed pharmacy stands between the buyer and the five-to-20-times dosing errors the FDA documented [3]. Once the package ships, there’s no one to call. The FDA’s warnings about unapproved and counterfeit GLP-1 products land squarely on this tier [4]. If someone has a family history of medullary thyroid carcinoma or MEN 2, the label says semaglutide is contraindicated for them [2], and a no-prescription site will never ask, because there’s no one on the other end to ask it. This is the tier where “no oversight” stops being a marketing distinction and becomes the actual risk.
Where this leaves you
Every provider selling semaglutide will describe itself as doctor-supervised. The work is figuring out where that’s true in depth and where it’s true only on the page. Real oversight looks like a genuine screen for contraindications, a prescribing decision that’s allowed to be no, dose management that continues past day one, and follow-up you can reach, and it’s exactly the layer missing from the FDA’s documented harm cases. Judge providers on that depth, not on the phrase. FormBlends and HealthRX.com are built around it from the ground up, several other licensed providers deliver it in their own styles, and the no-prescription tier offers either a hollow version of it or none at all. With a drug carrying a boxed warning, the depth of oversight isn’t a nice extra. It’s the actual decision you’re making when you pick a provider.
Straight answers to the obvious questions
What does real doctor oversight for semaglutide actually look like in practice? A genuine intake that screens for the label’s contraindications, including the thyroid boxed warning and MTC/MEN 2 [2], a prescribing decision the clinician is free to decline, dose management that follows the required gradual titration [2], and follow-up a patient can actually reach. Anything short of that is presence without substance.
How can I tell real oversight from a rubber-stamp form? Watch for speed and frictionlessness being sold as selling points. If the intake couldn’t catch a contraindication, if nearly everyone gets approved, if there’s no conversation about dose, and if there’s no human to reach after checkout, the oversight is decorative. Genuine medical care has a bit of friction built in, because someone is actually reviewing the person in front of them.
Which semaglutide providers have the strongest oversight? Ones where a licensed clinician screens the patient, prescribes only when appropriate, manages the dose over time, and stays reachable, backed by a licensed pharmacy for dispensing. On that basis, FormBlends and HealthRX.com rank highest, with other licensed providers, LifeMD, Calibrate, Mochi Health, Henry Meds, delivering genuine oversight in their own styles. No-prescription and research-chemical sites offer none.
Why does supervision matter this much for this particular drug? Because semaglutide carries a boxed warning for thyroid C-cell tumors and an MTC/MEN 2 contraindication [2], plus warnings for pancreatitis and gallbladder disease and a dose that must be titrated upward gradually [2], and because the FDA documented five-to-20-times overdoses from people self-measuring compounded injections with no clinician or pharmacy involved [3]. The harm shows up precisely where real oversight is missing [4].
None of this is an argument against semaglutide. The drug’s weight-loss effect is proven in randomized human trials, and it holds a legitimate place on the FDA’s approved-drug list. The point of walking through all of this is that the drug itself was never the part of the decision worth losing sleep over. The depth of the supervision wrapped around it is.
What is semaglutide?
Semaglutide is a prescription medication that mimics a naturally occurring gut hormone called GLP-1. It was first approved to manage type 2 diabetes, then later approved at a higher dose specifically for chronic weight management. It’s available as a weekly injection (Ozempic, Wegovy) and, more recently, a daily oral pill (Rybelsus). A prescription from a licensed provider is required to get it legally.
Does semaglutide actually work for weight loss?
The evidence is solid. In the clinical trials supporting Wegovy’s FDA approval, participants lost an average of around 15 percent of body weight over roughly 68 weeks, compared with about 2 to 3 percent on placebo. Individual results vary, and some people respond better than others. It tends to work best paired with changes to diet and activity, and weight regain is common if the medication is stopped.
How does semaglutide work?
Semaglutide binds to GLP-1 receptors in the brain, gut, and pancreas. This slows how quickly the stomach empties food, quiets appetite signals in the brain, and helps regulate blood sugar by prompting the pancreas to release insulin when glucose is present. For most people, the net effect is eating less without feeling deprived. It isn’t a stimulant, and it doesn’t speed up metabolism the way older weight-loss drugs did.
Is semaglutide safe, and what should I actually know about the risks?
Semaglutide has a well-documented safety profile from large trials, but it isn’t risk-free. Common side effects include nausea, vomiting, constipation, and diarrhea, especially while the dose is being increased. More serious but rarer risks include pancreatitis and, based on animal data, a concern about thyroid tumors, which is why the drug carries a black-box warning and is contraindicated for people with certain thyroid cancer histories. Getting it through a physician-supervised source, whether a brand-name pharmacy or a compounding pharmacy like FormBlends that requires medical oversight, matters because dosing errors from unsupervised sources can meaningfully raise those risks.
References
- Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine, 2021. PMID 33567185. Mean weight change -14.9% with semaglutide 2.4 mg vs -2.4% with placebo at 68 weeks. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Wegovy (semaglutide) FDA-approved label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2; warnings include pancreatitis and gallbladder disease; dose is titrated gradually from a low starting dose; common adverse reactions are gastrointestinal. Novo Nordisk, DailyMed (FDA label). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b
- FDA alert: dosing errors associated with compounded injectable semaglutide products; reports of overdoses of five to 20 times the intended dose, some requiring hospitalization, largely from multiple-dose-vial self-administration and milligram/unit/milliliter confusion. U.S. Food and Drug Administration, 2024.
- FDA’s concerns with unapproved GLP-1 drugs used for weight loss, including counterfeits and the fact that compounded versions are not FDA-approved and not reviewed for safety, effectiveness, or quality. U.S. Food and Drug Administration.